

Cellulite (Gynoid lipodystrophy in medical jargon) is the only word we have to describe the uneven pitted surface or dimpling of the skin commonly seen on the thighs of women. The appearance often is described to resemble the surface of an orange peel or that of cottage cheese. The term cellulite was first used by Alquin and Pavot in France to describe this condition. It is common in women, rarely seen in men and begins at various ages depending on body habitus, genetic makeup, etc. Most middle aged women have it. The remainder thinks they have it. As sure as a woman will grow breasts after puberty, she will get dimples and lumps on her skin. Cellulite affects only the buttocks, thighs and legs to about four inches above the knees. I see many patients requesting correction of their cellulite and an equal number of proposed treatments. These include aminophylline wraps, liposuction, liposuction with forked metal tubes to cut fascial strands to the skin and combinations of liposuction with lasers. None are truly effective.
If cellulite were solely due to the amount of fat present under the skin then men and women with the equal amounts of thigh fat would show similar degrees of cellulite. This is clearly not the case. Even very obese men rarely have cellulite but cellulite can even be seen in slender women with good muscle tone who exercise regularly. After weight loss surgery the majority of patients have an improvement in cellulite with weight loss, but the condition worsens for others. Cellulite is a complex condition, and treatments such as weight loss have variable effects on the improvement or worsening of this condition
CAUSES
There are many predisposing factors that contribute to cellulite development. These include:
* Gender: Due to the underlying structure of fat and connective tissue described below, women are more likely to develop cellulite.
* Heredity: Empirically, it has been found that the degree and presence of cellulite, as with body habitus, often is similar among females within the same family.
* Race: Caucasian and African-American women are more likely to develop cellulite than Asian women.
* Increased fat under the skin.
* Age: Women begin to develop cellulite after puberty as part of normal anatomical and physiological development. Cellulite increases in severity with aging as a reflection of the thinning of the skin.
Currently there is no cure or gold standard for treatment of cellulite. This is due in part to the minimal understanding of what exactly causes cellulite and poor therapeutic effectiveness of most available modes of treatment.
The outer skin is separated from the underlying muscle by a layer of fat. The fat has little strength therefore lying parallel to the skin throughout the fat layer is a sheet of connective tissue called superficial fascia. This fascia in turn is connected via finger like septal extensions through the fat to the overlying skin and underlying muscle. We call the superficial fascia and the septal extensions the superficial fascial system. This architecture helps hold the fat together and keep the skin from falling down like a loose sock.

In some areas the distance between skin, superficial fascia and muscle or bone is very small or adherent. It is this relationship that produces the normal body surface contours of creases, folds, valleys, plateaus, and bulges and allows for sliding of the different layers over the bone framework with body movement.

The black bands represent adherent areas. The gray zones represent areas of intermediate thickness. The white zones are areas with the greatest distance between components, the least adherent. Overly aggressive liposuction in these white zone areas always give bad results because after removal of the fat there is nothing to hold the skin in place. Since the skin can not shrink enough it just hangs there.
With age and sun damage, the entire skin-superficial fat-superficial fascial system unit relaxes and stretches, resulting in hanging soft tissues, pseudo-fat deposit deformity and cellulite. In men the superficial fascia is much thicker/denser than it is in women and the septal extensions are crosshatched lying oblique to the plane of the skin. In women the septal extensions are fewer and lie perpendicular to the skin surface. Looking from above the skin surface downward the tissues are arranged like a down quilt with fat cells between the threads and the thread lines of the quilt are equivalent to the finger like septal extensions. Thus in men the quilt seen from above would have more and thicker thread lines crisscrossing in more directions lying oblique to the plane of the skin and less space between the thread lines versus women with fewer thread lines that are perpendicular to the skin plane.

Notice that the thickness of the female thigh is much greater than the male thigh, the fat globules are larger and some of these fat cells protrude into the skin layer contributing to a pitted skin surface appearance.

The thicker fat layer and lower zone of adherence (below the pelvic bone) in women contributes to the female shape and predisposes women to cellulite. That is cellulite is to women what baldness is to men.
The hormonal cycles that women go through after puberty creating the menstrual cycle may contribute to the weakening of this superficial fascial system.
From this microscopic anatomy we can surmise 3 causes of the skin surface dimpling and a combination of them:
1. Swollen fat cells swell that push up into the overlying skin. Since the septal extensions are fixed or shrink with scarring and aging this creates a puckered appearance on the skin surface. This is also called primary cellulite, or cellulite of adiposity, is not amenable to surgery and is usually seen in younger women. It is present when the patient is supine and erect and is, therefore, not related to skin laxity or gravity.
septal extensions or shortening of these septa resulting in pitting of the overlying skin. This is easily treated by cutting the responsible septa.
3. Descent of the skin and fat that normally occurs with aging resulting in skin pitting due to the pull of septa whose length is unchanged. This is more common in women who have an inherently weaker fascial support system to hold the skin up. This problem is aggravated by smoking, sun damage, massive weight loss or gain, and in some cases after liposuction. This is also called secondary cellulite, or cellulite of laxity and is surgically correctable by lifting techniques that tighten both the skin and the superficial fascia system. It usually appears after 35 years of age and is present when the patient is standing but not when lying down. The appearance approves dramatically when the skin at the hip level is pinched to correct the laxity. The body areas with the least adherence between the skin, fat, superficial fascial system and bone or muscle will have the greatest degree of skin laxity.
4. some combination of the above 3
Now you can see why men rarely have cellulite and all of this can become more visible as the skin thins with aging. Diet and exercise may improve the appearance by shrinking the size of the fat cells in primary cellulite but cannot alter the structure of the superficial fascial system connecting the skin to the muscles through the fat and thus cannot eliminate cellulite in its entirety. The skin usually is incapable of shrinking once the superficial fascial system is damaged.
There are also 3 levels of cellulite severity

Level (1) the skin has to be pinched or muscles have to contract in order to see surface dimpling
———————

Level (2) cellulite is only visible when standing
———————-

Level (3) cellulite is visible when standing or sitting with raised and depressed areas and nodules
———————-
TREATMENTS
The market for cellulite-reduction devices in the United States was more than $47 million in 2008. It is projected to grow to $62 million by 2013. Therapeutic options to manage cellulite can be characterized as topical treatment, injected agents, non-invasive physical modalities and invasive physical modalities (surgery, lasers, liposuction…).
Topical management consists of gels, ointments, foams, creams and lotions applied to the skin surface. In 2008, 40 percent more anti-cellulite creams were introduced than the previous year. Most active ingredients, including antioxidants and blood vessel dilators, are included to increase blood flow and lymphatic drainage. Some irritate the skin to cause skin swelling and thereby camouflage the cellulite. Other agents may actually promote the breakdown of fat cells or attempt to locally increase cell metabolism. Some topical ingredients, such as vitamin C, and vitamin A derivatives have been included to stimulate circulation, and affect the superficial fascial system. Some have tried to increase the effectiveness of anti-cellulite creams by using bio-ceramic-coated neoprene garments to increase the penetration of the active ingredients in the various creams. The best subjective assessment, by the patients themselves, revealed that only 3 of 35 aminophylline cream-treated legs had their cellulite appearance improved after 12 weeks of treatment. There is no difference in fat metabolism in areas of cellulite vs. areas without cellulite. Thus, aminophylline, resveratrol and other such creams have no effect. Save your money and stay away from these.
Some creams contain anti-estrogen compounds usually derived from plants. These may prevent the onset or progression of cellulite by blocking the effects of body hormones on the superficial fascial system. Once the damage is done it is unlikely that these could be effective.
The direct injections of pharmacologic agents into the veins, or local infiltration just under the skin referred to as intradermotherapy or mesotherapy, has been used to breakdown fat cells in an attempt to improve the look of cellulite. My views on this are quite negative and are fully elucidated in my blog Mesotherapy, Lipo-Dissolve, or Injection Lipolysis
A 2006 published study postulated that if the anchoring connective tissue septae and/or enlarged fat cells could be destroyed by the enzyme, collagenase that the cellulite would be improved. This enzyme destroys collagen in the superficial fascial system. They showed improvement with just one injection of collagenase. Cellulite area was reduced by 77% by day 1 in comparison to baseline and the resulted lasted with reductions of 74% at 1 week, 89% at 1 month, 86% at 3 months and 76% at 6 months. The patient satisfaction score was 1.75 at 6 months (1= completely satisfied, 4= not satisfied) while weight and thigh circumference did not change. Side effects included injection area soreness, bruising and mild swelling that resolved within a week or two. As yet this has not been FDA approved and the treatment may be hard to control. This may end up making the problem worse by further destroying a stretched and weakened superficial fascial system.
Non-invasive physical modalities include non-invasive modalities such as Endermologie® (LPG Systems, Valence, France). Endermologie is a French-designed form of external mechanical deep-tissue massage that the Food and Drug Administration (FDA) has approved to diminish the appearance of cellulite. During the massage, suction is used to pull the skin into a handheld machine where the skin is compressed and rolled to increase blood and lymphatic flow and to modify the underlying connective tissue. This therapy is done in a series of 30- to 45-minute sessions over a period of months. The cellulite-minimizing effect of all forms of deep-tissue massage is temporary, and therapy must be continued to maintain results. The massage stimulates the body to thicken the superficial fascial system by laying down more collage and ruptures some fat cells. There has been no evidence to date whether or not after a certain number of treatments you can stop and will have permanent reduction of cellulite. For less severe forms of cellulite endermologie may turn out to be the treatment of choice.
Invasive physical modalities include surgery, laser and liposuction.
A new laser device recently approved by the FDA combines the rhythmic suction massage with superficial cooling and low-intensity 810-nanometer diode laser pulsation to treat cellulite. This technology, Tri-Active™ (Cynosure, Inc., Chelmsford, Mass.) was designed to increase lymphatic drainage, tighten skin by stimulating underlying muscles and fascia, and increase superficial blood flow, thereby reducing the appearance of cellulite. The treatment regimen mimics that of Endermologie, with greater emphasis directed toward the proposed microcirculation-impairment theory of cellulite formation.
Subcision is a simple surgical procedure that has been noted to improve moderate to severe cellulite. With the use of local anesthesia, this technique is performed by inserting a notched metal tube into the fat layer of the skin. The catheter then is manually moved in a repetitive motion parallel to the surface to physically break the connective tissue adhesions that tether the skin to the muscle. This should only be used for cause #2 listed above. Over use of this can cause the skin to sag with gravity creating other unsightly problems that may be impossible to fix.
Liposuction may decrease the appearance of cellulite by reducing local fat volume and by disrupting the fibrous bands that cause the dimpling appearance of the skin surface. The procedure will not, however, permanently eliminate cellulite. Liposuction removes fat, but doesn’t solve connective tissue or skin thickness issues that contribute to cellulite. My malpractice insurance carrier requires me to add the disclaimer that liposuction does not cure cellulite on my liposuction consent forms.
In 2005 lasers that were preferentially absorbed by fat were developed. Others have worked on radiofrequency removal of fat. Another proposed treatment was selectively heating the superficial fascial system basically cooking it to the point where it shrinks. This sounds great but in reality did not deliver as promised.
SmoothShapes is one machine recently promoted in Shape and InStyle magazines as a worthy weapon. This device combines massaging rollers with a laser and a light source that is meant to smooth skin and influence circulation. Another in-office machine garnering attention is VelaSmooth, which uses infrared light, radiofrequency and mechanical massage.
On February 2, 2011 Cynosure introduced Cellulaze, a Laser Device for the Long-Term Reduction of Cellulite. In the Cellulaze procedure is performed under a local anesthetic and involves the insertion of a small cannula — a narrow tube the size of the tip of a pen — under the skin. Laser is applied under the skin surface — typically the buttocks and thighs. The laser is purportedly diminishes the lumpy pockets of fat, releases the areas of skin depression and increases the elasticity and thickness of the skin. Patients reportedly require just one treatment. As of February 2011 FDA approval for use in the United States is pending. I am skeptical that this would work.
Patients in one U.S. study demonstrated an average increase in skin thickness of 23 percent and 27 percent at one month and one year, respectively, while skin elasticity increased an average of 32.5 percent at one month and 21 percent at one ye
The F.D.A. still accepts before-and-after photos as proof of a cellulite treatment’s effect, despite the fact that photos are easily manipulated. The lighting, the angle that someone’s leg is at in the picture — all those will affect the appearance of the dimpling. Pressing a palm down hard on the back of the thigh for a few seconds is enough to make cellulite pits appear shallower, at least for the seconds it takes to snap a photo. When the buttock is tensed or clenched, the cellulite on it will look worse. All of these methods have been used in photo ads to sell cellulite treatments.
Thigh buttock lifts or belt lipectomies (removal of a section of skin that lies under what is normally covered by underwear or a bathing suit) tighten both the skin and the superficial fascial system.

The photo on the left shows a woman with secondary cellulite or cellulite of laxity. The middle photo shows the degree of improvement achieved by lifting the skin and fat layers and verifies this is cellulite of laxity. The photo on the right shows the improvement achieved after a belt lipectomy surgery.
However I do not recommend this surgery unless there is very severe skin sagging and/or excess skin especially in younger women. The degree of improvement after surgery for simple cellulite does not warrant the severity of the surgery. Also the patient with excess skin will be much happier after surgery than the patient who just has some cellulite because the procedure cannot completely smoothen the skin surface. The superficial fascial system can stretch out further after the surgery so that the result diminishes over time but with lifestyle changes to maintain a level body weight the patient will not get excessive sagging skin again. For all of my abdominoplasty/tummy tuck patients I design the skin removal to achieve some tightening of the thigh with improvement in their cellulite. In those cases the primary reason for the surgery is the abdomen and as long as the abdomen looks good the patient is happy. Of course they are even happier with the thigh improvements. I will have to leave that for a future blog.
Here are photos of abdominoplasty patients in which you can see the improvement in the thighs after surgery.





February 6, 2012 addendum:
The FDA has cleared Cynosure’s Cellulaze Workstation for the treatment of cellulite and for commercial distribution. Small small protective tubes are placed in small cuts made in the skin under local anesthesia. The Cellulaze laser fiber is then threaded down the tubes to treat the affected areas. The laser disrupts the septal connections to the skin, destroys some of the fat cells and stimulates a process of increasing skin thickness and elasticity. Clinical data has shown that Cellulaze treatments can increase the thickness of the skin by 25% and increase the elasticity of the skin by 29% at 1 year after treatment. It is too soon to tell if the results will last more than 1 or 2 years. I am still skeptical because the process does not restore the superficial fascial septal system but rather destroys it.
November 29, 2012 addendum:
This webcast from the International Society of Aesthetic Plastic Surgeons sheds a very favorable light on the Cellulaze system. The key to success is choosing the right patient and doing the procedure correctly so you do not divide every septal connection to the skin and do not overheat any of the tissues. There were more than 1.25 million searches for Cellulaze on RealSelf in 2012, up 32% from 2011.
April 23, 2013 addendum:
XIAFLEX® (an FDA-approved version of the enzyme clostridial collagenase histolyticum) is FDA approved to treat adult Dupuytren’s contracture patients with a palpable cord. The medication is injected into the cord in the patient’s palm and melts it away. Now researchers at Stony Brook University in Long Island, New York are about to begin phase IIa placebo-controlled clinical trials injecting the same collagenase to break down the collagen that anchors cellulite dimples in order to even out skin irregularities. This could be the first FDA approved medication to treat cellulite.
The phase I pilot clinical trial of 10 women treated for cellulite on the back of their thighs showed an average 77% reduction of cellulite as soon as 1 day after the injection with maintenance of the result after 6 months, average 76% reduction of cellulite in the injected area at 6 months. Only minimal side effects such as bruising, soreness, and mild swelling, were reported shortly after the injection. After 6 months, the patients reported an average satisfaction score of 1.75 (1=completely satisfied, 4=not satisfied). This is a treatment I never would have though of doing or investigating.
November 22, 2013 addendum:
 The US Food and Drug Administration (FDA) just approved InMode Aesthetic Solutions’ new applicator, BodyFX, for body contouring and temporary cellulite reduction of the buttocks, abdomen, flanks, and thighs. The new clearance also includes treatment to relieve minor muscle aches and pains, and to temporarily boost blood circulation. The system uses vacuum suction, radio frequency energy, and high-efficiency pulses.
The US Food and Drug Administration (FDA) just approved InMode Aesthetic Solutions’ new applicator, BodyFX, for body contouring and temporary cellulite reduction of the buttocks, abdomen, flanks, and thighs. The new clearance also includes treatment to relieve minor muscle aches and pains, and to temporarily boost blood circulation. The system uses vacuum suction, radio frequency energy, and high-efficiency pulses.
In clinical trials, there was a 100% response rate, and the
average patient showed a 68% improvement in cellulite with an average
circumferential reduction of 3.58 cm. It is unclear to me how short a time temporary may be.
A new platform introduces upgraded features to reduce the number of
treatments required while increasing efficacy by adding vacuum suction to affect deeper layers of fat tissue and safety by adding temperature monitoring, smart controls with automatic cut-offs.
BodyFX has already received marketing approval in Canada, Europe,
Australia, and areas of Asia for the temporary reduction of cellulite.
July 1, 2015 addendum:
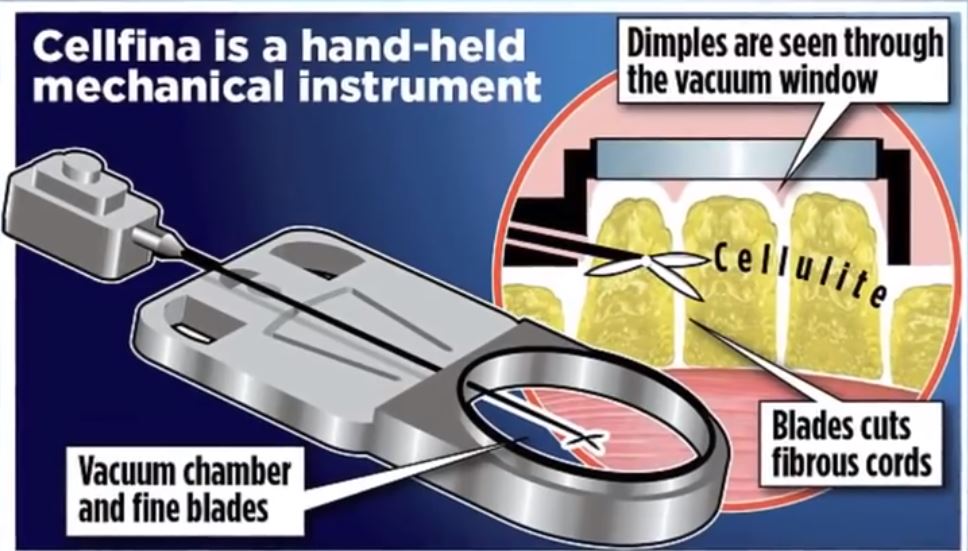
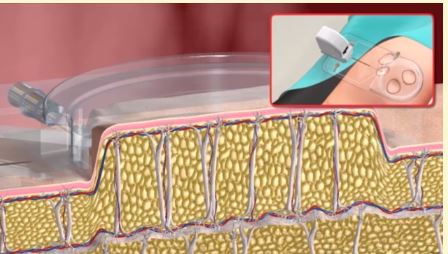
Another treatment is beginning to gain traction. Cellfina involves the placement of a vacuum chamber over the skin, injection of local anesthetic and introduction of a small rotating blade into the raised area to cut the bands causing cellulite. It is a fancy form of subcision but is approved by the FDA for long term, up to 1 year, resolution of buttock and thigh cellulite.
Surgical and Non-Surgical Treatment of Cellulite
Aaron Stone MD – Plastic Surgeon Los Angeles
Dr. Stone’s Twitter


![]()

![]()

Love your blog. Lots of info. I really want to take action on mine because it is very very bad. like stage 3.
thanks. keep at it please.