

- read about breast lift – mastopexy
- see before and after photos & videos
- alternatives, risks, benefits & recovery
Breast sagging or ptosis is usually treated surgically by removing excess skin resulting in a firmer breast. Because the problem is related to the skin and breast tissue (fat, breast gland and suspensory ligaments) rather than muscle this problem is unaffected by exercise. The cause of drooping is multifactorial:
- breast size
- genetic predisposition
- smoking history
- bra use history
- gravity
- age
- weight loss
- pregnancy with breast enlargement-engorgement and breast feeding
Whether a lift should be performed or not and what type of technique is used is dependent on the degree of drooping not the size of the breast. The nipple should be in line with or above the level of the infra-breast skin crease i.e. while standing upright the nipple should lie 20cm (about 8 inches) diagonally from the notch of the upper edge of the breast bone. For taller patients and those with severe drooping this point may be anywhere from 20 to 25cm. Lifting alone will not fill the upper half of the breast so some patients need this filling by either implants or fat grafting performed at the same time as the lift surgery. Historically breast lifts & augmentations performed at the same time were risky. With improved knowledge of blood supply they can be safely & reliably performed together to achieve results that are otherwise not possible.
All breast lifting procedures involve removal of breast skin. The pattern of skin removal for the lift depends on the amount of nipple lifting required. If the nipple lies only 2cm from the desired point a ring or donut of skin can be removed around the nipple areola complex thereby providing some lift with minimally visible scarring. For greater lengths of nipple elevation a lollipop or vertical incision is required. For even greater lengths where the nipples point downward toward the floor an inverted T or anchor shaped excision of skin is required. If the donut skin removal is attempted for greater amounts of lifting it will flatten the breast mound and resulted stretched areolae with significant scarring that me be impossible to fix.
Some surgeons place mashes under the skin or denude the surface skin and use it as a sling to prevent recurrent sagging. There is no evidence that doing so delays the recurrence of sagging so these are mostly marketing and selling ploys.


45 years old, 5’2″ tall, 125 lb., 38C bra size. This patient required a significant amount of lifting as is evident in the oblique view which shows the nipple was far below the infra-breast skin crease. Therefore an invert T or anchor pattern skin excision mastopexy was used to raise it up to the infra-breast skin crease level. The excision pattern is designed so that the scar is hidden under the breast when standing upright and is made asymmetric or not mirror imaged across a vertical plane through the nipple in order to achieve a natural appearance.
Breast lift mastopexy performed with inverted T closure. Breast implants were not placed.

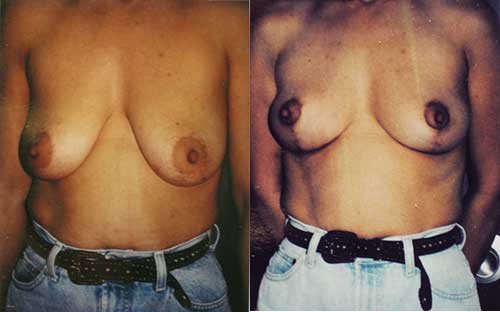
Breast lift mastopexy performed with inverted T closure in Afro-American patient. A small amount of breast tissue was removed on the left but this was basically a breast lift mastopexy without breast implant placement.

45 years old, 5′ tall, 120 lb., 36C bra size for breast lift with breast implant augmentation. This patient required a significant amount of lifting to raise the nipple 5.5cm (over 2 inches). The markings show the surgical plan. Black marks areas for skin removal. The upper red line marks the deep muscle incision so implant above the line will be under muscle and implant below the line will be superficial to muscle. The outer edges of the muscle are left intact to prevent implant shifting to the sides of the chest, a lateral dual plane. The implant was a 68 medium profile saline implant inflated to 360cc. The upper oblique red lines show the outer edge of the muscle. The lower oblique red lines show the pedicles for the nipple complexes to be rotated upward. The skin excision was an anchor or inverted T with a small horizontal skin excision above the crease. The result is 5 weeks after surgery.

43 years old, 5’5″ tall, 150 lb. African-American for breast lift with breast implant augmentation. This patient required a significant amount of lifting to raise the nipple 8cm (over 3 inches). The markings show the surgical plan. Black marks areas for skin removal. The upper red line marks the deep muscle incision so implant above the line will be under muscle and implant below the line will be superficial to muscle. The outer edges of the muscle are left intact to prevent implant shifting to the sides of the chest, a medial dual plane. The implants were saline, 375cc on the right and 330cc on the left, to improve symmetry. The upper oblique red lines show the outer edge of the muscle, the lower oblique red lines show the pedicles for the nipple complexes to be rotated upward and the red lines meeting in the middle show the level of the muscle cut for the medial dual plane. The skin excision was an anchor or inverted T with a small horizontal skin excision above the crease. The result is 5 weeks after surgery.
Video: Breast Lift With Fat Grafting
Video: Breast Lift With Saline Implant Breast Augmentation
Video: Breast Lift With Saline Implant Breast Augmentation
Read Dr. Stone’s blog about breast lift mastopexy surgeryBreast Lift – Boob Lift – Mastopexy
Internal Bra Breast Lift
Breast lift – mastopexy surgery can enhance your appearance and your self confidence. Realistic expectations are important to be happy with any surgery. As each patient is an individual, different results can be expected in each patient.
Alternatives
Although there are different surgical approaches there are no available alternatives to surgery.
Risks
The main risks of this surgery are skin scarring and recurrent drooping. The more drooping you have, the more skin you need to remove and the more skin scarring you will have. The pattern of skin removal is designed to hide the scars around the areola and in the crease under the breast but they can still be bothersome. The breast tissue is attached to the chest wall by Cooper’s ligaments and the increasing laxity of these ligaments allows the breasts to droop. The surgery however targets the stretched skin because we currently have no way to target the ligaments. The skin then re-stretches under the weight of the breasts which are no longer restrained from above by the ligaments. Some surgeons believe internal slings of mesh or denuded skin can counteract this but the mesh is either absorbable or its attachements loosen with time and the denuded skin is still skin so it stretches.
Benefits
The benefits are the self confidence of not seeing drooping breasts and being less self conscious when intimate. The outside world does not usually see the results of the surgery.
Recovery
Drains are not usually required and sutures are removed at 10 to 12 days. The most important part of recovery is exercise and activity restrictions for 3 to 4 weeks after surgery after which patients rapidly return to their pre-surgery exercise routines.
Dr. Aaron Stone
Call today for a consultation!
9700 Venice BlvdCulver City, Los Angeles,CA 90232
Many people who are interested in Plastic Surgery decide not to seek treatment because of the prices associated with cosmetic plastic surgery. What they may not know is that financing plans can help manage the costs and bring cosmetic surgery within the reach of nearly every budget.Many patients choose their cosmetic surgeon based on prices for plastic surgery rather than credentials. It is important to thoroughly research your doctor to ensure that he or she has the requisite training, experience, and facility. Making sure you get the results you desire the first time around could mean lower cosmetic surgery costs in the long run. Choosing an inexperienced surgeon could jeopardize your safety and result in health problems or the need for follow-up surgeries.Dr. Stone offers patients a range of payment options to help cover plastic surgery costs, including cash, check, and credit cards. In addition, he offers plastic surgery financing plans to help patients set up an affordable payment schedule by breaking up the costs of Plastic Surgery treatment into affordable monthly payments through
